Authors
Nil Albiol, Nuria Martínez-Cibrián, Andrea Franch, Almudena Navarro, A.ÁfricaMartín-López, Lucía López-Corral, Marta Español-Rego, Sergio Navarro, Leticia Alserawan, Irene Lopez-Oreja, Daniel Benitez-Ribas, FerranNadeu, Aina Oliver-Caldés, PabloMozas, Juan Gonzalo Correa, Andrea Rivero, Laura Magnano, Eva Giné, Elena Medina, Luis Gerardo Rodriguez-Lobato, Helena Brillembourg, Alexandra Martinez-Roca, Mercedes Montoro-Lorite, Pilar Ayora,Carla Ramos, Carlos Fernándezde Larrea, Sonia Rodríguez, Xavier Setoain, E.Azucena González-Navarro,Manel Juan, Armando López-Guillermo, Julio Delgado, Valentín Ortiz-Maldonado.
Introduction
Patients with CLL refractory to both BTK and BCL2 inhibitors show poor outcomes with no standard treatment available besides clinical trials. CD19-directed CAR-T can achieve complete responses even in those with high-risk genomics (i.e., TP53 aberrations). Still, few patients attain long-term remissions with currently approved products (median PFS around 12 months), and their availability worldwide is scarce. Additionally, those presenting with Richter’s transformation (RT) have no CAR-T products approved for.
We report the results of our academic CD19-directed CAR-T product (varnimcabtagene autoleucel, or ARI-0001) in patients with R/R CLL or RT.
Methods
This study included subjects with CLL or RT treated with ARI-0001 in the CART19-BE-01 trial (NCT03144583) and in the subsequent compassionate use program.
ARI-0001 is an autologous, CD19-directed, second-generation 4-1BB costimulated CAR-T product fully developed at Hospital Clínic (Barcelona, Spain) currently approved in Spain for the treatment of R/R B-cell acute lymphoblastic leukemia. Patients were infused in single or fractionated dosing (10%, 30%, and 60%) with 0.1-1.0 or 0.5-5.0 x10e6 ARI-0001 cells/kg (CLL or RT, respectively), after lymphodepleting chemotherapy with fludarabine 30 mg/m2/d and cyclophosphamide 300 mg/m2/d on days -6 to -4.
Results
We included 29 patients treated with ARI-0001 between 2017 and 2024, 13 with CLL and 16 with RT. The median age was 60 years (range 29-78), 11 (38%) were female. Patients had received a median of 3 prior lines (range 2-7). Virtually all had been previously exposed to ibrutinib (97%) and 20 (69%) to venetoclax. Most cases with RT (94%) had received prior R-CHOP as frontline therapy. Five RT individuals had also undergone previous allogeneic stem cell transplantation. The population was comprised of mostly high-risk patients, including 19 (90%) with unmutated IGHV, 21 (78%) with TP53 aberrations, and 11 (50%) with complex karyotype. The CLL cohort included 7 patients (54%) with Binet C stage; eleven had a CLL-IPI of ≥4 (85%). Regarding the RT cohort, 9 patients (58%) were stage IV and 11 (69%) showed elevated LDH values. Five cases were clonally related, the others were unknown.
Bridging therapy was employed in all patients but one (one RT): in CLL usually BTKi (30.4%) or venetoclax with (22.7%) or without ibrutinib (30.8%), while in RT chemotherapy regimens with (20.1%) or without ibrutinib (20.1%). All but two (1 CLL and 1 RT) received ARI-0001 in a fractionated manner.
The median vein-to-vein time was 35 days (29-50); ARI-0001 was manufactured in a median of 8 days (IQR 7-8). Most patients received the full target dose of ARI-0001 (62%). Although 90% of the patients developed cytokine release syndrome (CRS) only 3.4% were grade 3 or higher. Nineteen (66%) patients received tocilizumab, and 9 (31%) steroids for their CRS. There were only two cases (6.9%) of neurotoxicity (ICANS), all of them grade ≤2, treated with steroids. Median time to CRS and ICANS onset was 1 (IQR 1-3) and 7 days (IQR 1-13), respectively.
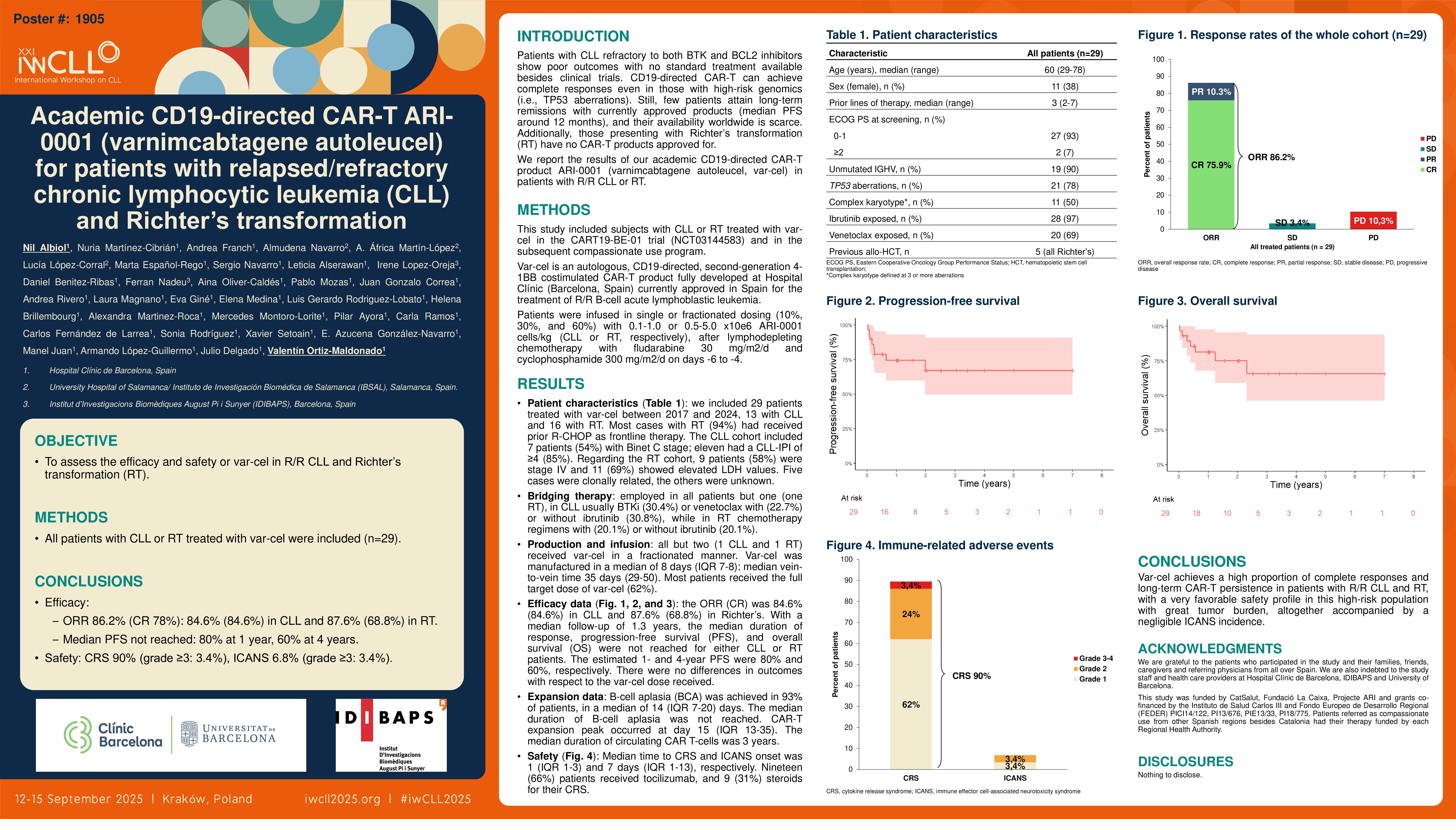
The overall response rates (ORR) and complete response rates (CR) in the entire cohort were 86.2% and 75.9%, respectively; in the CLL cohort, the ORR (CR) was 84.6% (84.6%), and in Richter’s 87.6% (68.8%). With a median follow-up of 1.3 years, the median duration of response, progression-free survival (PFS), and overall survival (OS) were not reached for either CLL or RT patients. The estimated 1- and 4-year PFS were 80% and 60%, respectively. There were no differences in outcomes with respect to the ARI-0001 dose received. The median duration of B-cell aplasia was not reached, and no difference was seen between CLL and RT. It was achieved in 93% of patients, in a median of 14 (IQR 7-20) days. CAR-T expansion peak occurred at day 15 (IQR 13-35). The median AUC (0-30d) for complete responders was significantly higher (28.79 vs 6.59, p=0.03), indicating that non-responders showed lower var-cel expansion, with no differences between CLL and RT. In fact, patients who did not reach CR exhibited inferior outcomes than those who did (mOS 4.7 months, p< 0.0001). The median duration of circulating CAR T-cells was 3 years.
Conclusions
ARI-0001 achieves a high proportion of complete responses and long-term CAR-T persistence in patients with R/R CLL and RT, with a very favorable safety profile in this high-risk population with great tumor burden, altogether accompanied by a negligible ICANS incidence.
Keywords : CAR-T, ARI-0001, var-cel
Please indicate how this research was funded. : None
Please indicate the name of the funding organization.: