Authors
XiaoJie Yan MD, PhD, Gonzalo Blanco PhD, Shreya Sanghani, Anna Puiggros PhD, Steven Allen MD, Jonathan Kolitz MD, Goutamie Sukhram, Hatice Gur, Sadia Morium, Anessa Jeetoo, Kelli Pote, Blanca Espinet PhD, Kanti Rai MD, Nicholas Chiorazzi MD.
Background
Monoclonal B-cell lymphocytosis (MBL) is a common finding in the aging population, with a reported average prevalence of 15% in individuals between age 40 to 100 years. MBL is divided to 2 categories, lcMBL ( < 500 cells/ul), which represent ~95% of cases, and hcMBL (500-4,999 cells/ul), representing ~ 5% of cases. Since people with hcMBL progress to CLL at rate of ~5% per year, identifying those people with hcMBL who will progress to CLL is very important clinically reasons and studying this process could allow pre emptive, preventive therapy. Although random population-based studies provide valuable information about MBL prevalence, developing a screening approach that would favor finding people with hcMBL would be more valuable for studying the natural history and understanding the pathobiology of this disorder. Here we show that focusing on individuals with persistent absolute lymphocytosis (PAL) offers a targeted strategy for identifying hcMBL, thereby allowing studies to improving our understanding of this pre-leukemic condition.
Methods
This study investigated the prevalence and characteristics of MBL within a well-defined cohort of patients with PAL. We define PAL as an absolute lymphocyte count (ALC) consistently above 3.3 x 10^9/L for at least 90 days. All participants underwent multiparameter flow cytometry analysis using a comprehensive panel of antibodies targeting B-, T-, and myeloid-cell markers.
Results
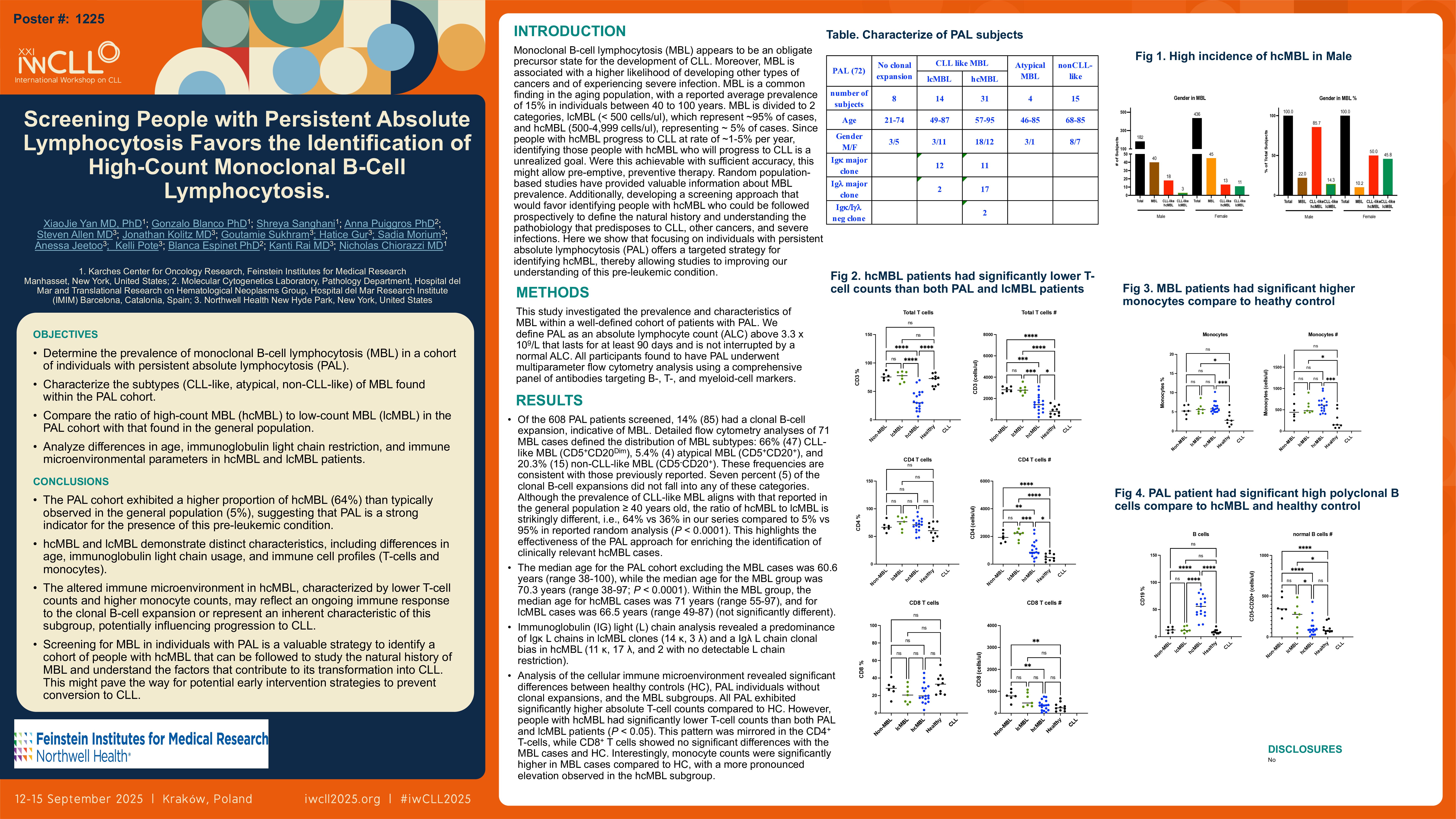
Of the 608 PAL patients screened, 14% (85) had a clonal B-cell expansion, indicative of MBL. Detailed flow cytometry analysis of 71 MBL cases allowed us to determine the distribution of MBL subtypes: 66% (47) CLL-like MBL (CD5+CD20Dim), 5.4% (4) atypical MBL (CD5+CD20+), and 20.3% (15) non-CLL-like MBL (CD5-CD20+). These frequencies are consistent with those previously described. Seven percent (5) of the clonal B-cell expansions did not fall into any of these categories. Although the prevalence of CLL-like MBL aligns with that reported in the general population ≥ 40 years old, the ratio of hcMBL to lcMBL is strikingly different, i.e., 64% vs 36% in our series compared to 5% vs 95% in the reported random analysis (P < 0.0001), highlighting the effectiveness of the PAL approach for enriching the identification of clinically relevant MBL cases.
The median age for the PAL cohort excluding the MBL cases was 60.6 years (range 38-100), while the median age for the MBL group was 70.3 years (range 38-97; P < 0.0001). Within the MBL group, the median age for hcMBL cases was 71 years (range 55-97), and for lcMBL cases was 66.5 years (range 49-87) (not significant).
Moreover immunoglobulin (IG) light (L) chain analysis revealed a predominance of Igκ L chains in lcMBL (14 κ, 3 λ) and a Igλ L chain bias in hcMBL (11 κ, 17 λ, and 2 with no detectable L chain restriction).
Analysis of the cellular immune microenvironment revealed significant differences between healthy controls (HC), PAL individuals without clonal expansions, and the MBL subgroups. All PAL exhibited significantly higher absolute T-cell counts compared to HC. However, people with hcMBL had significantly lower T-cell counts than both PAL and lcMBL patients (P < 0.05). This pattern was mirrored in the CD4+ T-cells, while CD8+ T cells showed no significant differences with the MBL cases and HC. Interestingly, monocyte counts were significantly higher in MBL cases compared to HC, with a more pronounced elevation observed in the hcMBL subgroup.
Discussion
Our findings demonstrate a significantly higher prevalence of hcMBL among people with PAL than estimated for the general population. In addition, the observed differences in age, Ig L chain use, and T and monocyte numbers between lcMBL and hcMBL underscore the distinct clinical and biological characteristics of these subgroups. Moreover, the elevated T-cell and monocyte counts observed in hcMBL might reflect an ongoing immune response to the expanding clonal B-cell population or evidence for an immature, precursor population bearing oncogenic mutations. Thus, screening people with PAL is an effective strategy to identify clinically relevant, hcMBL cases, to allow an understanding of the natural history of this condition and define the molecular and immunologic processes that influence its conversion to CLL.
Keywords : Lymphocytosis, high-count monoclonal B-cell lymphocytosis, microenvironment
Please indicate how this research was funded. :
Please indicate the name of the funding organization.: