Authors
Scott F. Huntington, Justin T. Puckett, Beenish S. Manzoor, Sophia Li, Yves Paul Mbous, Carolina Reyes, Nnadozie Emechebe, Sachin Kamal-Bahl, Holly Budlong, Jalpa A. Doshi.
Introduction
Over the last decade, the treatment landscape for chronic lymphocytic leukemia (CLL) has shifted significantly with the introduction of novel therapies such as treat-to-progression Bruton’s tyrosine kinase inhibitors (BTKis) and fixed-duration BCL-2 inhibitors (BCL-2is). Though BTKis and BCL-2is (venetoclax) have largely supplanted traditional chemotherapy in treatment guideline recommendations, little is known about utilization of these novel therapies and how it varies by age, race/ethnicity, and income. Furthermore, overall survival and associated factors in the real-world setting are poorly understood. Real-world evidence is especially lacking in patients covered under Medicare, a federal insurance program covering most older adults and representing the largest payer for CLL-related care in the U.S.
Aim
To examine access to novel therapies, overall survival, and associated factors in a national sample of fee-for-service U.S. Medicare beneficiaries initiating CLL treatment in the frontline setting
Methods
This retrospective cohort study used 2016-2023 100% Medicare fee-for-service claims, identifying beneficiaries age ≥65 years initiating treatment for frontline CLL between 6/1/2019 and 12/31/2022. The index date was the date of the first prescription fill or infusion. Novel therapies included BTKis (ibrutinib-, acalabrutinib-, or zanubrutinib-based regimens) and BCL-2is (venetoclax-based regimens); all other CLL treatments (anti-CD20 monotherapy, traditional chemotherapy, etc.) were classified as non-novel. Novelty of CLL treatment received (BTKi/BCL-2i [novel] vs. other [non-novel]) was examined in the overall sample and by key subgroups defined by age (65-69, 70-74, 75-79, 80+), race/ethnicity (White, Black, Hispanic, Other), and Part D low-income subsidy (LIS) status (LIS duals, LIS non-duals, and non-LIS). Among novel treatment users, we further examined treatment type by duration (treat-to-progression BTKis vs. fixed-duration BCL-2i), overall and by key subgroups. Kaplan-Meier curves for overall survival [OS] were generated in the overall sample, by CLL treatment received, and by key subgroups of interest. Binomial logistic regressions and Cox regressions were used to examine the association of key sociodemographic factors with novel treatment utilization and OS, respectively, while controlling for other patient demographic, clinical, and insurance plan characteristics.
Results
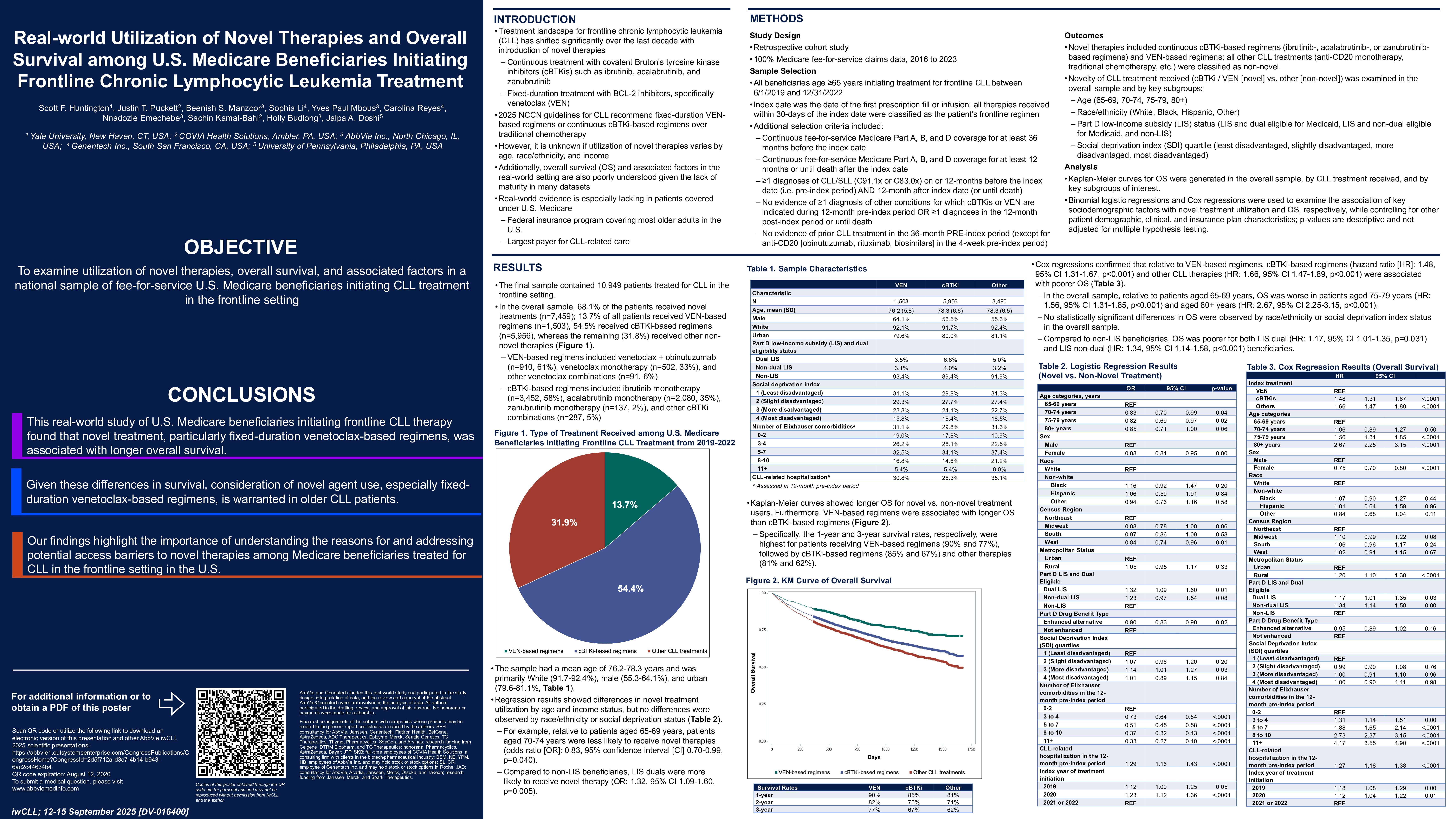
The final sample contained 10,949 patients treated for CLL in the frontline setting. In the overall sample, 68.1% of the patients received novel treatments (n=7,459); 13.7% of all patients received fixed-duration venetoclax (n=1,503), 54.5% received BTKis (n=5,956), whereas the remaining (31.8%) received other non-novel therapies. Descriptive results showed differences in novel treatment utilization by age and income status, but no differences were observed by race/ethnicity. Regression results confirmed these findings. For example, relative to patients aged 65-69 years, patients aged 75-79 years were less likely to receive novel therapies (odds ratio [OR]: 0.82, 95% confidence interval [CI] 0.69-0.98, p=0.030). No statistically significant differences in receipt of novel therapies or fixed-duration treatment were observed by race/ethnicity. Compared to non-LIS beneficiaries, LIS duals were more likely to receive novel therapy (OR: 1.32, 95% CI 1.09-1.60, p=0.005).
Kaplan-Meier curves showed longer OS for novel vs. non-novel treatment users. Furthermore, venetoclax was associated with higher OS than BTKis. Specifically, the 1-year and 3-year survival rates, respectively, were highest for patients receiving venetoclax (90% and 77%), followed by BTKis (85% and 67%) and other therapies (81% and 62%). Cox regressions confirmed that relative to venetoclax use, BTKi (hazard ratio [HR]: 1.49, 95% CI 1.32-1.68, p< 0.001) and other CLL therapies (HR: 1.65, 95% CI 1.46-1.87, p< 0.001) use were associated with poorer OS. In the overall sample, relative to patients aged 65-69 years, OS was worse in patients aged 75-79 years (HR: 1.55, 95% CI 1.30-1.84, p< 0.001) and aged 80+ years (HR: 2.66, 95% CI 2.25-3.15, p< 0.001). No statistically significant differences in OS were observed by race/ethnicity in the overall sample. Compared to non-LIS beneficiaries, OS was poorer for both LIS dual (HR: 1.15, 95% CI 1.00-1.33, p=0.049) and LIS non-dual (HR: 1.34, 95% CI 1.14-1.58, p< 0.001) beneficiaries.
Conclusion
This national real-world study of Medicare beneficiaries initiating frontline CLL therapy found that novel treatment, particularly the BCL-2i venetoclax, was associated with longer overall survival. Given these differences in survival, consideration of novel agent use, especially venetoclax combinations, is warranted in older CLL patients. Our findings highlight the importance of understanding the reasons for and addressing potential access barriers to novel therapies among Medicare beneficiaries with CLL in the U.S.
Keywords : CLL, venetoclax, survival/overall survival
Please indicate how this research was funded. : AbbVie and Genentech funded this real-world study and participated in the study design, interpretation of data, and the review and approval of the abstract. AbbVie/Genentech were not involved in the analysis of data. All authors participated in the drafting, review, and approval of this abstract. No honoraria or payments were made for authorship.
Please indicate the name of the funding organization.: AbbVie and Genentech