Authors
Catherine C. Coombs, Lindsey E. Roeker, Joanna M. Rhodes, Nilanjan Ghosh, Beenish S. Manzoor, Nicole Lamanna, Toby A. Eyre, Jennifer R. Brown, Nnadozie Emechebe, Hande H. Tuncer, Nancy Kaddis, Chaitra Ujjani, Lori A. Leslie, Brian T. Hill, Alan P. Skarbnik, Paul M. Barr, Frederick Lansigan, Matthew S. Davids, Christopher E. Jensen, Nicolas Martinez-Calle, Wendy Sinai, Laurie Pearson, Zhu Cui, Michael Coyle, Bita Fakhri, Meghan C. Thompson, Deborah M. Stephens, Andres Chang, Samin Houshyar, Irina Pivneva, Talissa Watson, Annie Guerin, Mazyar Shadman
Introduction
Clinical trials have demonstrated deep responses and extended survival with venetoclax-based therapy (VEN) in patients with high-risk (i.e., unmutated IGHV [uIGHV] and/or del[17p]/TP53) CLL/SLL). However, real-world data on clinical outcomes for patients with high-risk CLL/SLL are still limited or constrained by short follow-up durations.
Objectives
This study evaluated clinical outcomes in patients who initiated VEN in first-line (1L) or second-line (2L) settings as mono- or combination therapy and had high-risk CLL/SLL.
Methods
Data on adult patients with CLL/SLL from 25 sites of the CLL Collaborative Study of Real-World Evidence (CORE), a global, retrospective, observational study were used. Patients included had del(17p)/TP53 and/or uIGHV prior to initiation of VEN in 1L or 2L. Clinical outcomes assessed were overall response rate (ORR; proportion of patients with a documented physician-defined complete/partial response), progression-free survival (PFS; time from VEN initiation to disease progression/death or end of follow-up), time to next treatment/death (TTNT-D; time from VEN initiation to subsequent treatment/death or end of follow-up), and overall survival (OS; time from VEN initiation to death or end of follow-up).
Outcomes were reported by high-risk feature (non-mutually exclusive: del[17p]/TP53; uIGHV; uIGHV-only (i.e., without confirmed del[17p/TP53]); both uIGHV+del[17p]/TP53), line of therapy (1L, 2L), including further by high-risk feature, and VEN regimen (monotherapy [VMono]; combination [VCombo]). Kaplan-Meier methodology was used to estimate 24-month rates.
Results
Of 2,696 patients in CORE, 317 patients (11.8%) with high-risk CLL/SLL initiated VEN and were included (1L: 206 [65.0%]; 2L: 111 [35.0%]). Among the 317 patients (median age: 64.9 years), 87 (27.4%) had del(17p)/TP53 (1L: 39 patients; 2L: 48 patients), 272 (85.8%) had uIGHV (1L: 191 patients; 2L: 81 patients), 221 (69.7%) had uIGHV-only (1L: 159 patients; 2L: 62 patients), and 42 (13.2%) had both uIGHV+del(17p)/TP53 (1L: 24 patients; 2L: 18 patients). VMono was initiated by 45 (14.2%) patients, while 272 (85.8%) received VCombo (mostly with obinutuzumab: 199 [73.2%]). Among patients who initiated VEN in 2L, common 1L therapy included ibrutinib- (26/48 [54.2%]), CT/CIT- (9 [18.8%]), and rituximab-based therapy (4 [8.3%]). Median follow-up was 24.0 (IQR: 11.1, 37.8) months (median VEN duration of 11.1 [IQR: 8.2, 13.2] and 13.6 [IQR: 5.7, 24.6] months in 1L and 2L, respectively).
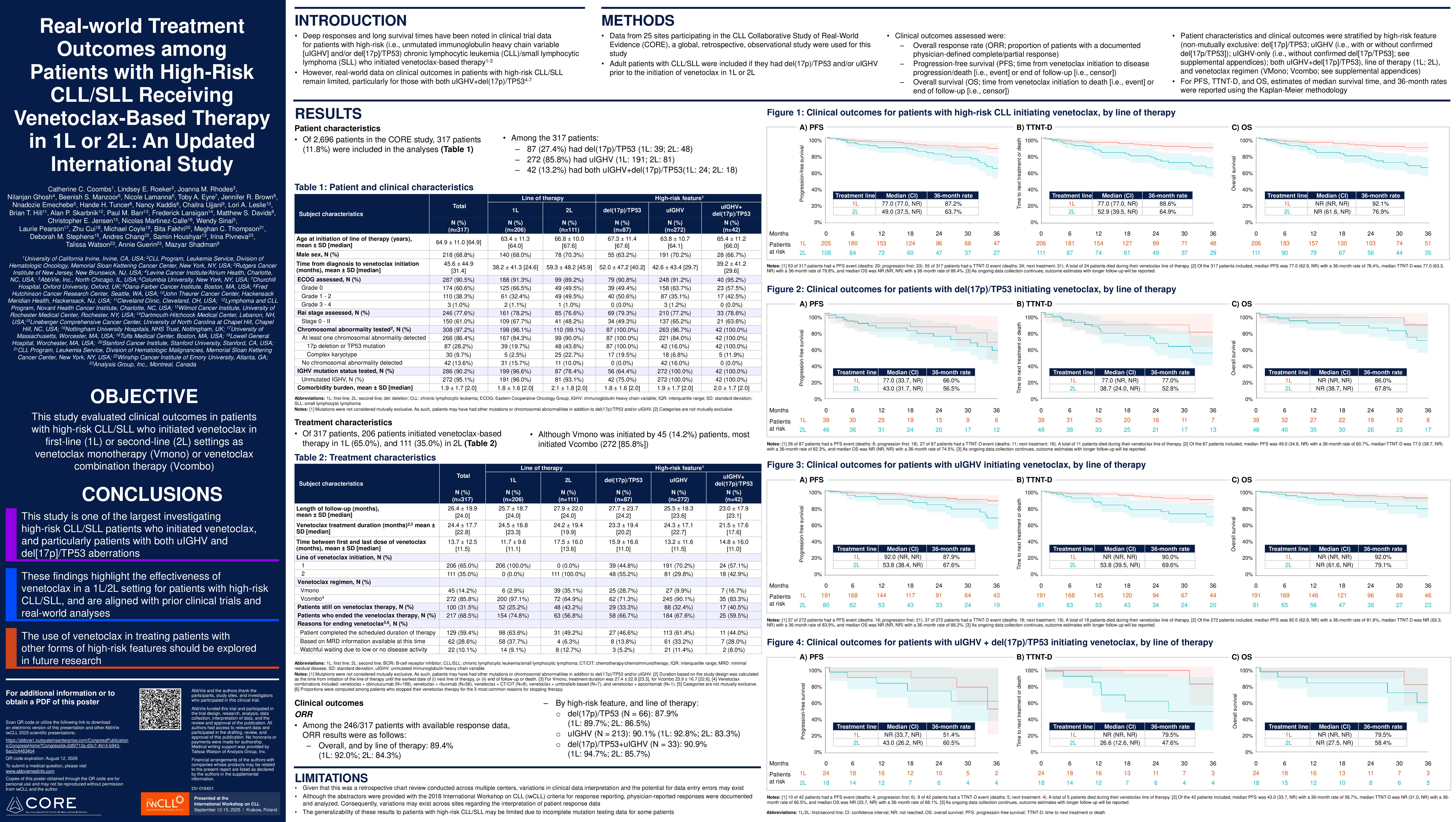
In 87 patients with del(17p)/TP53, ORR was 87.9% with 24-month rates of 77.6% for PFS, of 74.5% for TTNT-D, and of 87.5% for OS. In 272 patients with uIGHV, ORR was 90.1% with 24-month rates of 89.4% for PFS, of 88.3% for TTNT-D, and of 92.6% for OS. In 221 patients with uIGHV-only, ORR was 91.9% with 24-month rates of 91.5% for PFS, of 91.3% for TTNT-D, and of 93.0% for OS. In 42 patients with both uIGHV+del(17p)/TP53, ORR was 90.9% with 24-month rates of 81.0% for PFS, of 78.8% for TTNT-D, and of 89.1% for OS.
In 1L, ORR was 92.0% (del(17p)/TP53: 89.7%, uIGHV: 92.8% among 142 patients, uIGHV-only: 94.5% among 120 patients, uIGHV+del(17p)/TP53: 94.7% among 18 patients) with 24-month rates of 90.8% for PFS (del(17p)/TP53: 84.0%, uIGHV: 91.8%, uIGHV-only: 92.6%, uIGHV+del(17p)/TP53: 88.1%), of 90.9% for TTNT-D (del(17p)/TP53: 85.5%, uIGHV: 92.5%, uIGHV-only: 93.5%, uIGHV+del(17p)/TP53: 95.5%), and of 94.4% for OS (del(17p)/TP53: 94.6%, uIGHV: 94.5%, uIGHV-only: 94.2%, uIGHV+del(17p)/TP53: 95.5%).
In 2L, ORR was 84.3% (del(17p)/TP53: 86.5%, uIGHV: 83.3%, uIGHV-only: 84.4%, uIGHV+del(17p)/TP53: 85.7%) with 24-month rates of 80.6% for PFS (del(17p)/TP53: 72.9%, uIGHV: 83.5%, uIGHV-only: 88.3%, uIGHV+del(17p)/TP53: 72.6%), of 75.9% for TTNT-D (del(17p)/TP53: 66.8%, uIGHV: 78.0%, uIGHV-only: 85.3%, uIGHV+del(17p)/TP53: 59.4%), and of 86.3% for OS (del(17p)/TP53: 82.4%, uIGHV: 87.8%, uIGHV-only: 89.6%, uIGHV+del(17p)/TP53: 81.7%).
In patients who initiated VMono, ORR was 72.7% with 24-month rates of 75.7% for PFS, of 68.1% for TTNT-D, and of 83.7% for OS. In patients who initiated VCombo, ORR was 92.0% with 24-month rates of 89.2% for PFS, of 88.9% for TTNT-D, and 93.0% for OS.
Conclusion
This is one of the largest studies to date on VEN use in high-risk CLL/SLL, particularly for those with both uIGHV+del[17p]/TP53. These results, which build on previous findings from clinical trials and real-world data, demonstrate the clinical effectiveness of VEN in 1L/2L for treatment of patients across high-risk features (i.e., uIGHV and/or del[17p]/TP53). Future research should continue to investigate the use of VEN in treating patients with high-risk CLL/SLL.
Keywords : treatment effectiveness, high-risk, BCL2i
Please indicate how this research was funded. : This study was funded by AbbVie. AbbVie contributed to its design, and the collection, analysis, and interpretation of the data. AbbVie participated in the writing, review and approval of the poster content in collaboration with the other authors. All authors contributed to the development of the publication and maintained control over the final content.
Please indicate the name of the funding organization.: AbbVie