Authors
Constantine S. Tam, Paolo Ghia, Mazyar Shadman, Talha Munir, Stephen S. Opat, Patricia A. Walker, Masa Lasica, Ian W. Flinn, Tian Tian, Stephanie Agresti, Jamie Hirata, Jennifer R. Brown.
Background
Zanubrutinib is a next-generation Bruton tyrosine kinase inhibitor that is approved for five indications, including chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). Initial results from the SEQUOIA study (NCT03336333), at a median follow-up of 26.2 months, demonstrated superior progression-free survival (PFS) by independent review with zanubrutinib vs bendamustine + rituximab (arms A and B) in patients with treatment-naive (TN) CLL/SLL without del(17p) as well as high overall response rate (ORR) and PFS benefit in patients with del(17p) (arm C). Additionally, the 5-year follow-up in arm A demonstrated durable PFS benefit, with estimated 54- and 60-month PFS rates of 80% and 76%, respectively. Here we report updated results in SEQUOIA arm C, in patients with del(17p), after approximately 5 years of follow-up (data cutoff: Apr 30, 2024).
Methods
Arm C is a nonrandomized cohort of SEQUOIA patients with del(17p) that received zanubrutinib monotherapy. Investigator-assessed PFS, overall survival (OS), ORR, and safety/tolerability were evaluated. Adverse events were recorded until disease progression or start of next-line therapy.
Results
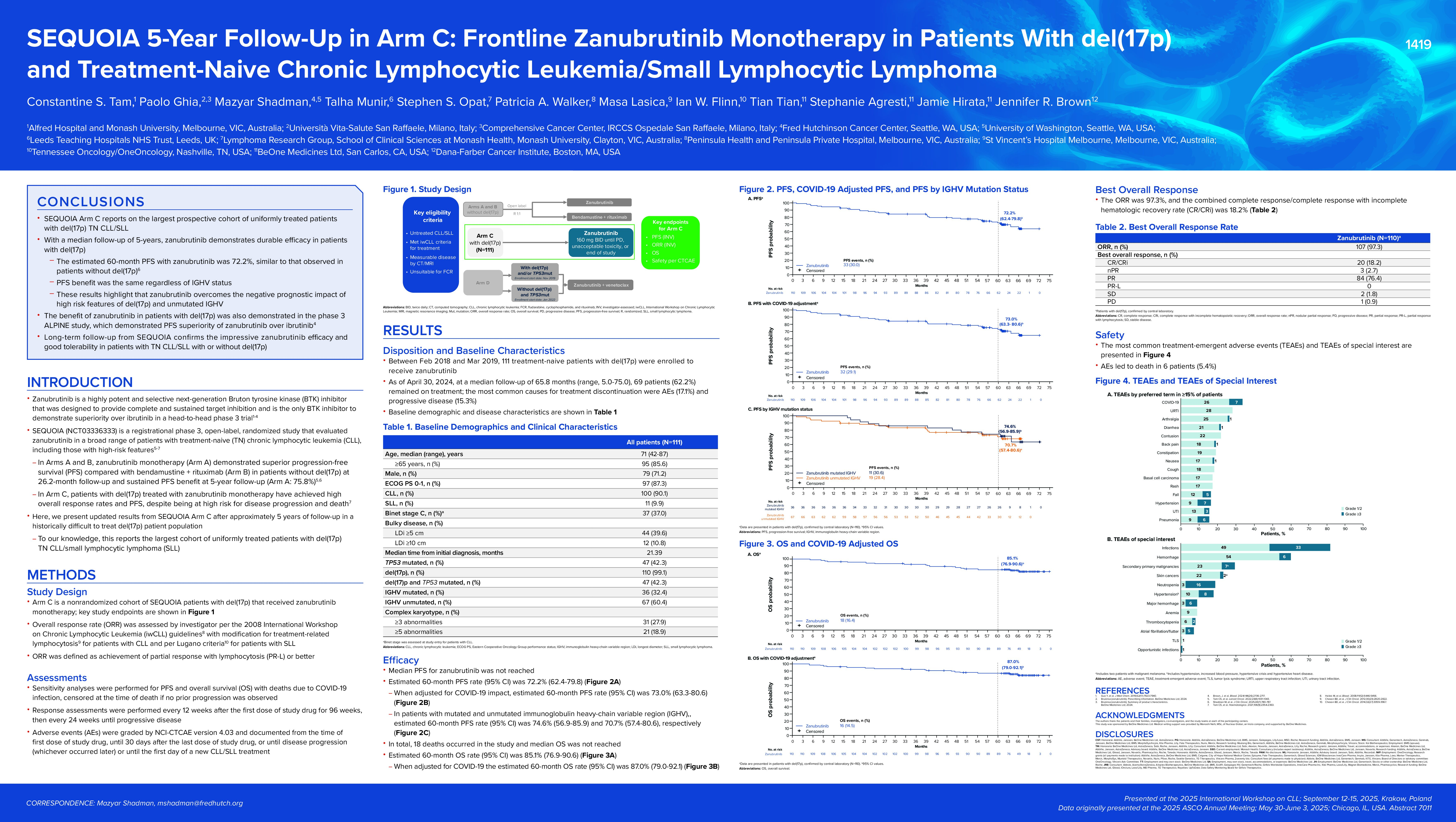
Between Feb 2018 and Mar 2019, 111 TN patients with del(17p) were enrolled to receive zanubrutinib. The median age was 71 years (range, 42-87), 79 (71%) were male, 67 (60%) were IGHV unmutated, and 47 (42%) had both del(17p) and TP53 mutation. At a median follow-up of 65.8 months (range, 5-75), median PFS was not reached. The estimated 60-month PFS rate was 72.2% (62.4%-79.8%), or 73.0% (63.3%-80.6%) when adjusted for COVID-19. Median OS was also not reached. The estimated 60-month OS rate was 85.1% (76.9%-90.6%), or 87.0% (79.0%-92.1%) when adjusted for COVID-19. The ORR was 97.3%, and the complete response/complete response with incomplete hematologic recovery rate was 18.2%. Zanubrutinib treatment was ongoing in 62.2% of patients. The most common causes for treatment discontinuation were adverse events and progressive disease (in 17.1% and 15.3%, respectively). Key adverse events of interest (AEI) included any-grade infection (82%), bleeding (60%), neutropenia (19%), hypertension (18%), anemia (9%), thrombocytopenia (8%), and atrial fibrillation/flutter (7%). Grade ≥3 AEI included infection (33%), neutropenia (16%), hypertension (8%), bleeding (6%), atrial fibrillation/flutter (5%), and thrombocytopenia (2%).
Conclusions
With this 5-year follow-up in SEQUOIA, the efficacy of zanubrutinib in TN higher-risk patients with del(17p) was maintained and patients continue to demonstrate PFS benefits consistent with the randomized cohort of patients without del(17p) (arm A). Additionally, with longer-term follow-up, no new safety signals were identified. This update, in the largest cohort of uniformly treated patients with del(17p), suggests that zanubrutinib remains a valuable frontline treatment option for patients with or without del(17p) CLL/SLL. Updated data from a more recent data cut-off will be available for the presentation.
Keywords : Zanubrutinib, CLL, Treatment-naive
Please indicate how this research was funded.:
Please indicate the name of the funding organization. : BeOne Medicines Ltd