Authors
Tahla Munir, Rhys Williams, David Campbell, Swetha Challagulla, Qianhong Fu, Mei Xue, Keri Yang, Andrew H. Lipsky.
Introduction
Bruton tyrosine kinase inhibitors zanubrutinib and ibrutinib have demonstrated efficacy in the first-line (1L) chronic lymphocytic leukemia (CLL) setting in SEQUOIA (NCT03336333) and RESONATE-2 (NCT01722487) trials, respectively, while the efficacy and safety of zanubrutinib and ibrutinib were compared in patients receiving second-line or later (2L+) treatment in the phase 3 ALPINE trial (NCT03734016). However, there are limited real-world head-to-head comparative data on cardiac deaths of patients being treated with zanubrutinib and ibrutinib. The objective of this study was to conduct a modeling analysis to estimate the number of cardiac deaths in the US that could be avoided by using zanubrutinib instead of ibrutinib for 2L+ CLL treatment based on published head-to-head data from ALPINE. Additionally, an exploratory analysis was conducted to investigate the number of cardiac deaths that could be avoided with 1L use of zanubrutinib vs ibrutinib.
Methods
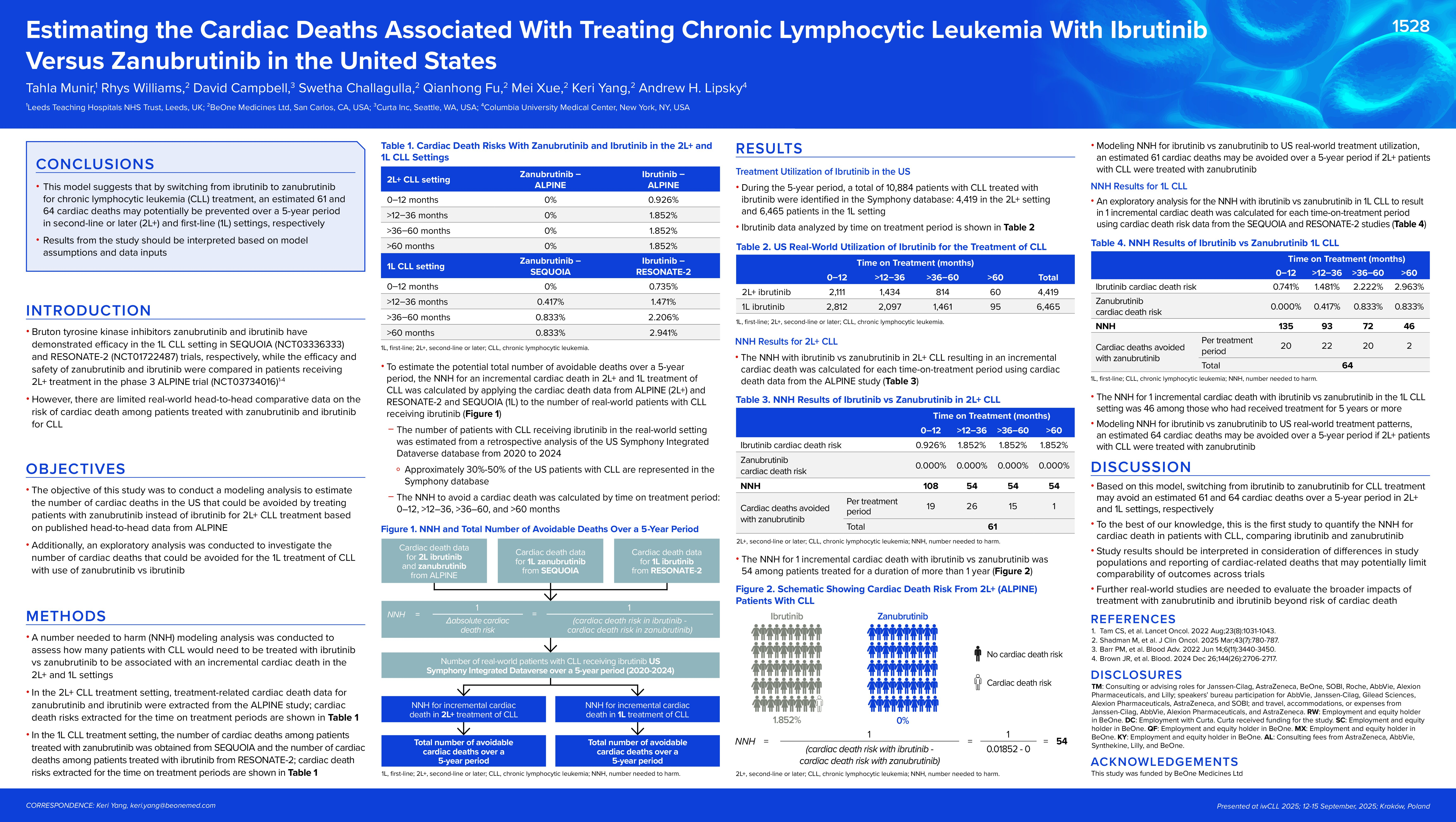
A number needed to harm (NNH) modeling analysis was conducted to assess how many patients would need to be treated with ibrutinib vs zanubrutinib to be associated with an incremental cardiac death in the 1L and 2L+ settings. Rates of cardiac deaths for zanubrutinib and ibrutinib in 2L+ CLL were extracted from the ALPINE study (0% for zanubrutinib vs 1.852% for ibrutinib) and SEQUOIA (0% for zanubrutinib) and RESONATE-2 (2.941% for ibrutinib). NNH was calculated as the reciprocal of the absolute cardiac death risk increase for ibrutinib when compared with zanubrutinib (1/ [cardiac death risk in ibrutinib – cardiac death risk in zanubrutinib]). The number of CLL patients receiving ibrutinib in the real-world setting was estimated from a retrospective analysis of the US Symphony Integrated Dataverse database from 2020 to 2024. To estimate the potential total number of avoidable deaths over a 5-year period, NNH for incremental cardiac death in 2L+ and 1L treatment of CLL was calculated by applying the risks of cardiac death data from ALPINE (2L+) and RESONATE-2 and SEQUOIA (1L) to the number of real-world CLL patients receiving ibrutinib.
Results
The model used published trial data and real-world CLL patient numbers for NNH analysis. A total of 10,884 CLL patients treated with ibrutinib were identified in the Symphony database, with 6,465 patients in 1L setting, and 4,419 in 2L+ setting. The NNH model estimated that in 2L+ setting up to 61 cardiac deaths may be avoided over a 5-year period in the US if 2L+ CLL patients were treated with zanubrutinib instead of ibrutinib. Additionally, for every 54 patients treated with ibrutinib instead of zanubrutinib for R/R CLL, one additional cardiac death occurred over five years. Exploratory NNH analysis of the 1L setting suggested that up to 84 deaths may be avoided a 5-year period if CLL patients were treated with zanubrutinib instead of ibrutinib. Over this same period, for every 34 patients treated with ibrutinib instead of zanubrutinib one additional cardiac death occurred.
Conclusion
This model suggests that by switching from ibrutinib to zanubrutinib for CLL treatment, an estimated 61 and 84 cardiac deaths may potentially be prevented over a 5-year period in 2L+ and 1L settings, respectively. Results from the study should be interpreted based on model assumptions and data input. Further real-world studies are needed to evaluate the broader impacts beyond cardiac death from treatment with ibrutinib over zanubrutinib.
Keywords : CLL, BTKi, cardiac deaths
Please indicate how this research was funded. : BeOne Medicines Ltd.
Please indicate the name of the funding organization.: BeOne Medicines Ltd.