Authors
Emilia Jaskuła, Anna Sobczyńska-Konefał, Wojciech Szlasa, Monika Kisielewska, Robert Mroczek, Marta Szyca-Śmieszniak, Monika Mordak-Domagała, Jacek Kwiatkowski, Katarzyna Tatara, Agnieszka Kuś, Mateusz Sawicki, Izabela Dereń-Wagemann, Mariola Sędzimirska, Marzena
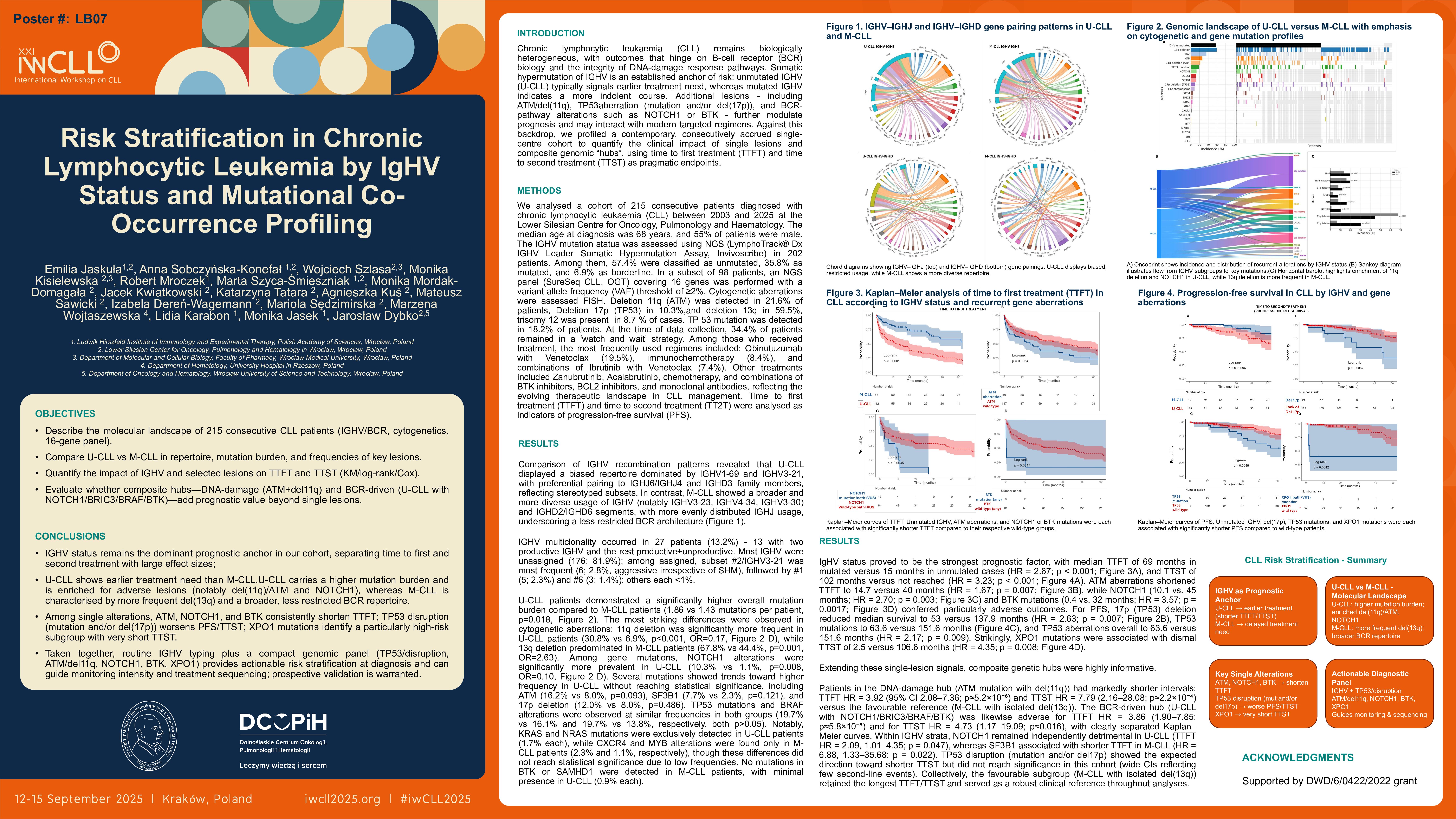
Comprehensive molecular characterisation of chronic lymphocytic leukaemia (CLL) enables precise prognosis and personalisation of treatment. We analysed 215 consecutive patients (median age: 68 years; 55% male) diagnosed between 2003 and 2025 at the Lower Silesian Centrer for Oncology, Pulmonology and Haematology. IgHV mutation status was determined in 202 patients (62% unmutated, 38% mutated), and cytogenetic changes were assessed by FISH. In 98 patients, an NGS panel covering 16 genes was performed with a VAF threshold of ≥2%. Time to first treatment (TTFT) and time to second treatment (TT2T) were analysed as a measure of progression-free survival (PFS). Co-occurrence of variants was analysed using Fisher’s test and hierarchical clustering.
IgHV status proved to be the strongest prognostic factor. The median TTFT was 69 months in the M-CLL group and 17 months in the U-CLL group (HR = 2.66; p < 0.001), and TT2T was 150.5 and 102.7 months, respectively (HR = 2.46; p = 0.008). The 17p (TP53) deletion had a significant impact on PFS. In patients with this alteration, the median PFS was 53 months (95% CI: 32.4–NA), compared to 137.9 months (95% CI: 102–NA) in the others (HR = 0.38; p = 0.006). The differences were already apparent after 24 months and confirmed by 1-, 3- and 5-year survival analysis (log-rank p = 0.0047), where 5-year PFS was 38% in the group with 17p deletion vs. 76% without it.
The analysis revealed a significant correlation between 11q (ATM) deletion and unmutated IgHV status — this aberration was present in 31% of U-CLL cases, compared to 7% in M-CLL (p = 0.0002). Additionally, TP53 mutations significantly correlated with the presence of 17p deletion (r = 0.73; p < 0.001), indicating a consistent phenotype of DNA repair pathway damage.
The use of unsupervised cluster analysis (K-means, k = 5) allowed for the identification of five biologically and clinically distinct subgroups of patients:
• BRAF/NOTCH1 cluster (4.7%): characterised by the presence of BRAF and NOTCH1 mutations; characterised by the shortest time to treatment (TTFT: 10.6 months) and the second shortest progression-free survival (PFS: 26.1 months).
• High-risk cluster (13.0%): dominated by NOTCH1, SF3B1 and BRAF mutations; patients in this group had the second shortest TTFT (11.0 months) and the shortest PFS (16.8 months).
• TP53/17p cluster (8.4%): includes patients with a high frequency of 17p deletions (100%) and TP53 mutations (94%); the median TTFT was 14.8 months and the PFS was 28.3 months.
• Standard cluster (67.4%): represents a mixed molecular profile, with the most common 13q deletion (54%); TTFT was 19.7 months and PFS was 29.4 months.
• Favourable cluster (6.5%): characterised by the lowest percentage of unfavourable mutations and the absence of 17p deletion; patients in this group had the longest time to treatment (TTFT: 22.9 months) and the best prognosis (PFS: 38.5 months).
These results confirm that co-occurrence analysis and a cluster approach enable precise differentiation of CLL phenotypes with different clinical courses, supporting personalised treatment and optimal clinical trial design.
Keywords : CLL, IGHV, TP53
Please indicate how this research was funded. : Supported by DWD/6/0422/2022 grant
Please indicate the name of the funding organization.: