Authors
Alexey Danilov, Stephen Rosen, Sandra Thomas, Dongyun Yang, Tanya Siddiqi, Sandra Ortega-Francisco, Maria Teresa Aquino, Flavia Chiuppesi, Miguel-Angel Gutierrez, Jing Li, Jada Mack-Onyeike, Jacqueline Miller, Yifei Zhou, Tony Le, Jennifer Johnson, Corinna La Rosa, Qiao Zhou, Teodora Kaltcheva, Angela Patterson, Shannon Dempsey, Katrin Tiemann, Kelly McKee, Felix Wussow and Don J. Diamond.
Patients (pts) with CLL have impaired immune responses to vaccination and are at increased risk for infections, including SARS-CoV-2. Pt’s inability to mount effective antibody responses to vaccinations is caused by both disease-related immune suppression and treatments which negatively impact B cell function. Hence, a vaccine which could induce a strong cellular immune response warrants investigation in CLL. GEO-CM04S1 is a Modified Vaccinia Ankara-based vaccine which expresses both Spike (S) and Nucleocapsid (N) SARS-CoV-2 antigens, the former known to have high variability.
Aim
To evaluate immune response following administration of GEO-CM04S1 vaccine in CLL pts.
We conducted a 1:1 randomized observer-blinded phase 2 trial in pts with CLL (NCT05672355). Pts received two doses of either Pfizer/BioNTech mRNA (with XBB.1.5 S sequence) (Ctrl) or GEO-CM04S1 (Exp; expressing the Wuhan S and N) vaccine on day(d) 1 and d84 of the study. Primary endpoint was T cell immune response at d56 post-injection of either vaccine. Secondary endpoints included safety, the duration/magnitude of T cell response, Th1/Th2 polarization, S- and N-specific IgG levels and neutralizing antibodies levels against SARS-CoV-2 variants up to d365. Simon 2-stage design was used to suspend accrual in an arm after interim analysis if T cell immune response results in that arm was disappointing.
We enrolled 31 pts (16 on Exp and 15 on Ctrl arm) who received a median of 1 prior therapy (range, 1-8); 52% were men. Two pts (1 per arm) withdrew from the study before receipt of first dose. All pts exhibited moderate baseline serum S-specific IgG levels, with no significant change post-vaccine. Pts form both arms mounted a significant increase in RBD-specific IgG response on d28; and on d84 in the Ctrl arm. Predictably, only the Exp arm showed a 2-4-fold increase in the level of N-specific IgG post-vaccination. Neutralizing antibodies against the ancestral strain Wuhan (D614G) and Omicron variants (BA.1 and XBB.1.5) were present in both arms and reached a statistically significant increase at d28 for Omicron BA.1.
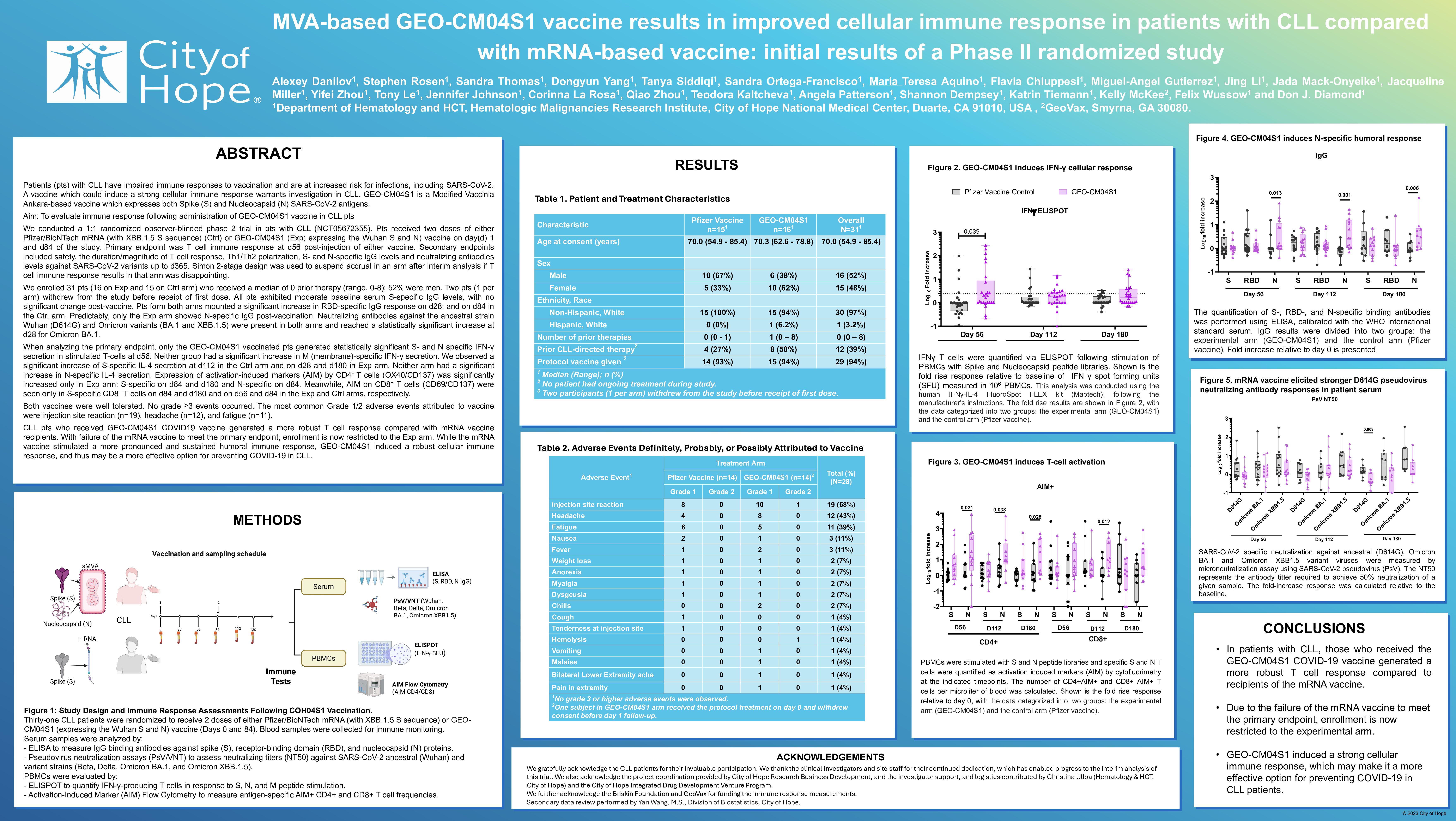
When analyzing the primary endpoint, only the GEO-CM04S1 vaccinated pts generated statistically significant S- and N specific IFN-γ secretion in stimulated T-cells at d56. Neither group had a significant increase in M (membrane)-specific IFN-γ secretion. We observed a significant increase of S-specific IL-4 secretion at d112 in the Ctrl arm and on d28 and d180 in Exp arm. Neither arm had a significant increase in N-specific IL-4 secretion. Expression of activation-induced markers (AIM) by CD4+ T cells (OX40/CD137) was significantly increased only in Exp arm: S-specific on d84 and d180 and N-specific on d84. Meanwhile, AIM on CD8+ T cells (CD69/CD137) were seen only in S-specific CD8+ T cells on d84 and d180 and on d56 and d84 in the Exp and Ctrl arms, respectively.
Both vaccines were well tolerated. No grade ≥3 events occurred. The most common Grade 1 adverse events were injection site reaction (n=19), fatigue (n=12) and cough (n=10).
CLL pts who received GEO-CM04S1 COVID19 vaccine generated a more robust T cell response compared with mRNA vaccine recipients. With failure of the mRNA vaccine to meet the primary endpoint, enrollment is now restricted to the Exp arm. While the mRNA vaccine stimulated a more pronounced and sustained humoral immune response, GEO-CM04S1 induced a robust cellular immune response, and thus may be a more effective option for preventing COVID-19 in CLL.
Keywords : Covid-19, vaccine, T-cell
Please indicate how this research was funded. :
Please indicate the name of the funding organization.: