Authors
Tong-lu Qiu, Yi Xia, Shuhua Yi, Chun Qiao, Huayuan Zhu, Yuting Yan, Wei Xu, Lu-gui Qiu, Jian-yong Li.
Objective
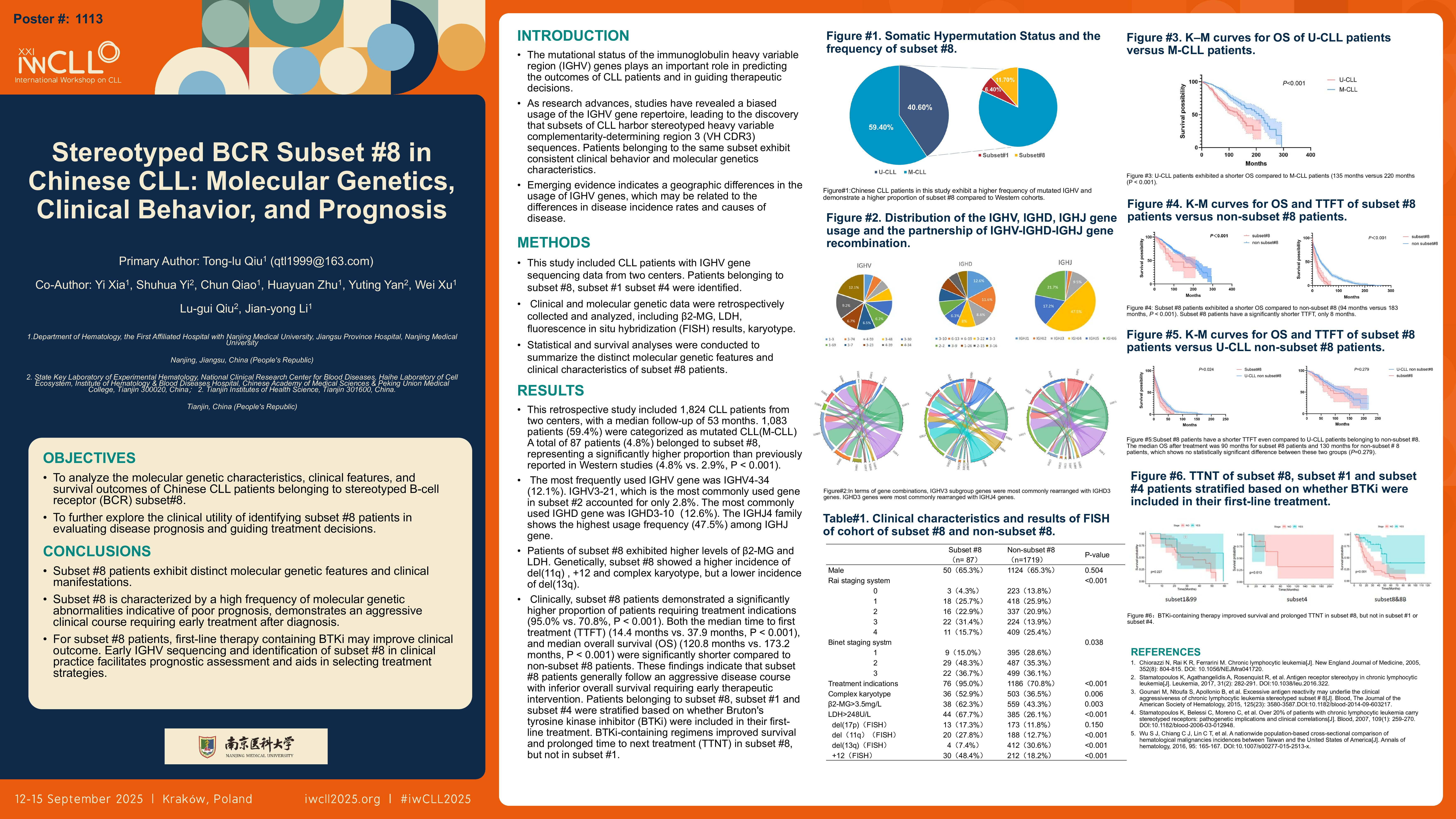
To analyze the molecular genetic characteristics, clinical features, and survival outcomes of Chinese chronic lymphocytic leukemia (CLL) patients belonging to stereotyped B-cell receptor (BCR) subset #8 (including its satellite subset #8b; collectively referred to as subset #8), and to further explore the clinical utility of identifying subset #8 patients in evaluating disease prognosis and guiding treatment decisions.
Methods
This study included CLL patients with available immunoglobulin heavy variable (IGHV) gene sequencing data from two centers: the First Affiliated Hospital of Nanjing Medical University and Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Sciences. Patients belonging to subset #8, subset #1 (including its satellite subset #99, collectively referred to as subset #1), and subset #4 were identified. Clinical and molecular genetic data were retrospectively collected and analyzed, including β2-microglobulin (β2-MG), lactate dehydrogenase (LDH), fluorescence in situ hybridization (FISH) results, karyotype (using CpG-oligonucleotide and interleukin-2 stimulation), and next-generation sequencing (NGS) results. Statistical and survival analyses were conducted to summarize the distinct molecular genetic features and clinical characteristics of subset #8 patients, as well as their prognostic differences compared with non-subset #8 patients. The probability of progression-free survival (PFS) and overall survival (OS) was estimated by using Kaplan-Meier method and the differences between the survival curves of different groups of patients were assessed by using the log-rank test.
Result
This retrospective study included 1,824 CLL patients from two centers, with a median follow-up of 53 months. Among these patients, 1,083 patients (59.4%) were categorized as mutated CLL(M-CLL) and 741 patients (40.6%) as unmutated CLL(U-CLL). A total of 87 patients (4.8%) belonged to subset #8, representing a significantly higher proportion than previously reported in Western studies (4.8% vs. 2.9%, P < 0.001). Compared to non-subset #8 patients, patients of subset #8 exhibited higher levels of β2-microglobulin (β2-MG) (4.67 mg/L vs. 3.81 mg/L, P = 0.004) and lactate dehydrogenase (LDH) (416.7 U/L vs. 231.9 U/L, P < 0.001). Genetically, subset #8 showed a higher incidence of del(11q) (27.8% vs. 12.7%, P = 0.001), trisomy 12 (+12) (48.4% vs. 18.2%, P < 0.001), and complex karyotype (52.9% vs. 36.5%, P = 0.006), but a lower incidence of del(13q) (7.4% vs. 30.6%, P < 0.001). Clinically, subset #8 patients demonstrated a significantly higher proportion of patients requiring treatment indications (95.0% vs. 70.8%, P < 0.001). Both the median time to first treatment (TTFT) (14.4 months vs. 37.9 months, P < 0.001), and median overall survival (OS) (120.8 months vs. 173.2 months, P < 0.001) were significantly shorter compared to non-subset #8 patients. These findings indicate that subset #8 patients generally follow an aggressive disease course with inferior overall survival requiring early therapeutic intervention. Patients belonging to subset #8, subset #1 and subset #4 were stratified based on whether Bruton’s tyrosine kinase inhibitor (BTKi) were included in their first-line treatment. BTKi-containing regimens improved survival and prolonged time to next treatment (TTNT) in subset #8, but not in subset #1. Analysis of NGS results of paired pre-treatment and post-treatment suggested that BTKi-based first-line treatment reduced clonal evolution risk in subset #8 compared to chemoimmunotherapy (CIT), though BTKi resistance mutations remained a concern.
Conclusion
Subset #8 patients exhibit distinct molecular genetic features and clinical manifestations. Subset #8 is characterized by a high frequency of molecular genetic abnormalities indicative of poor prognosis, demonstrates an aggressive clinical course requiring early treatment after diagnosis. For subset #8 patients, first-line therapy containing BTKi may improve clinical outcome. Early IGHV sequencing and identification of subset #8 in clinical practice facilitates prognostic assessment and aids in selecting treatment strategies.
Keywords : Chronic lymphocytic leukemia; Immunoglobulin heavy variable region; Stereotyped BCR
Please indicate how this research was funded. :
Please indicate the name of the funding organization.: