Authors
Mercedes Borge, Chiara Cassarino, Valeria Sarapura Martinez, Alicia Díaz, Pablo Morande, Romina Gamberale, Mirta Giordano, Fernando Bezares.
Infectious complications represent a major cause of morbidity and mortality in CLL due to both, intrinsic immune dysfunction and detrimental effects of anti-leukemic therapies on the patient´s immune system. Hypogammaglobulinemia is the most common immune defect. Its prevalence ranges between 20 and 70% depending on the cohort analysed, with a decrease of all immunoglobulin (Ig) isotypes usually starting with IgM, then IgG and IgA (Freeman, Crassini et al. 2013, Parikh, Leis et al. 2015, Andersen, Vojdeman et al. 2016, Ishdorj, Streu et al. 2019). The administration of immunoglobulin replacement therapy (IgRT) is not recommended as routine prophylaxis, and is only reserved for patients with severe recurrent infections in the presence of hypogammaglobulinemia (Hallek, Cheson et al. 2018). Remarkably, Ig preparations used in CLL contain more than 95% IgG and as a result, IgA and IgM deficiencies persist unaddressed. An analysis of the factors associated with infections in CLL patients showed a stronger association between major infections and combined Ig deficiency rather than isolated IgG deficiency (Visentin, Compagno et al. 2015), thus an enriched Ig preparation may offer enhanced benefits. Moreover, we have previsoulsy reported that in contrast to standard IgRT, IgA- and IgM-enriched IVIg (IVIg-GAM) preparation showed a significantly lower inhibitory effect on T cells, a feature highlighted as a potential benefit of this particular preparation with the potential to preserve T cell function when administered in vivo (Khan, Molica et al. 2022). This study evaluates the impact of IVIg-GAM on infection rates and antimicrobial use in a small cohort of CLL patients.
We have conducted a retrospective analysis on six CLL patients who initiated IVIg-GAM (Pentaglobin) between 2018 and 2022. Patients were followed for 24 months. IVIg-GAM was administered at 400 mL every 25–28 days. All patients met local criteria for IgRT due to hypogammaglobulinemia (IgG < 400 mg/dL) and/or recurrent infections (≥3 per year). Data on infection episodes, antimicrobial use, and Ig levels were collected.
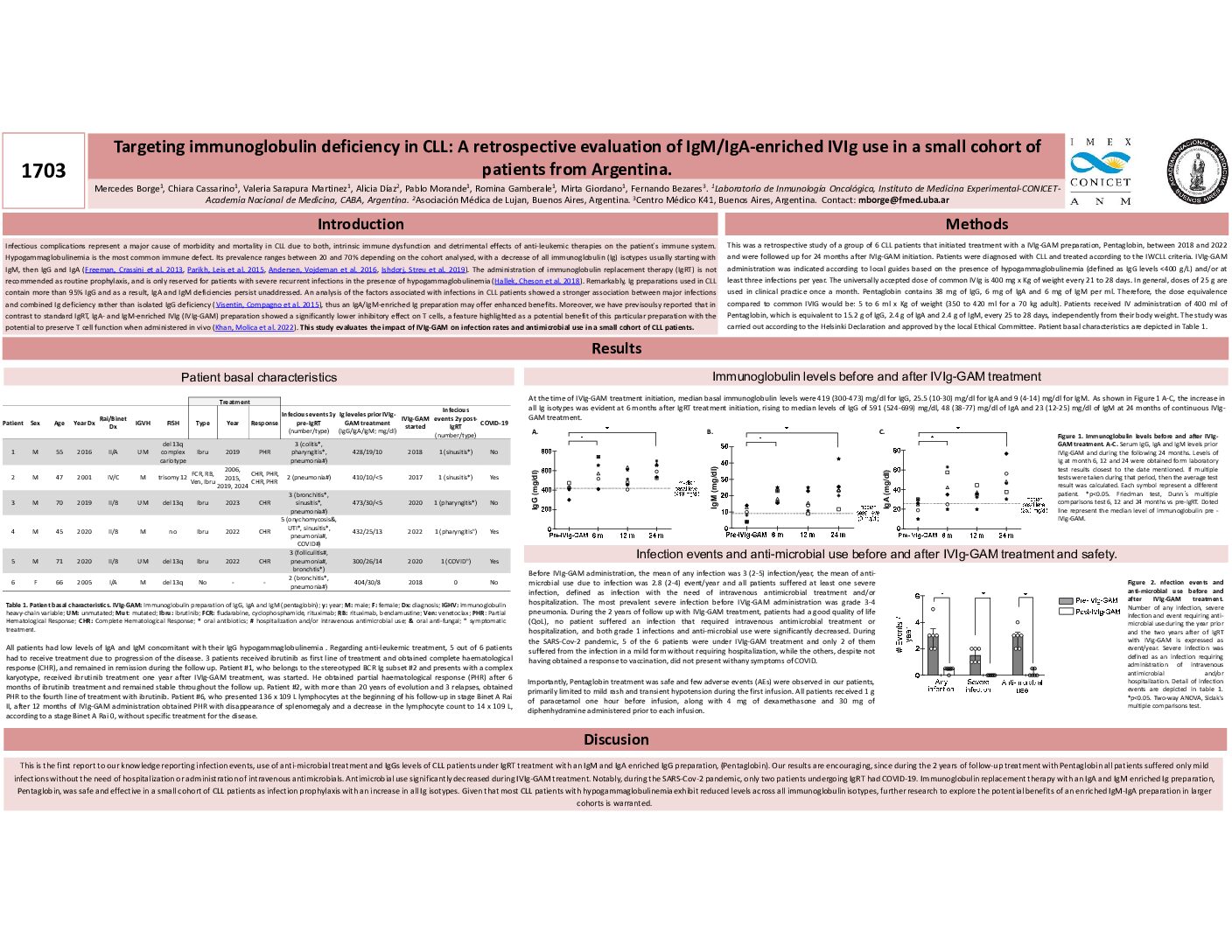
All patients exhibited low baseline levels of IgG, IgA, and IgM. Median baseline immunoglobulin levels were: IgG 419 mg/dL, IgA 25.5 mg/dL, and IgM 9 mg/dL. IVIg-GAM treatment led to a sustained increase in all Ig isotypes over 24 months, with median levels reaching: IgG 591 mg/dL, IgA 48 mg/dL, and IgM 23 mg/dL (p < 0.05. Friedman test, Dunn´s multiple comparisons test 6 and 24 months vs pre-IgRT). Prior to IVIg-GAM, patients experienced a mean of 3 infections/year and required antimicrobial therapy 2.8 times/year, with at least one severe infection requiring hospitalization. The most common severe infection was pneumonia. During IVIg-GAM treatment, no patient required hospitalization for infection, and both minor infections and antimicrobial use significantly decreased (p < 0.05. Two-way ANOVA, Sidak’s multiple comparisons test). During the COVID-19 pandemic, five patients were on IVIg-GAM; two contracted mild SARS-CoV-2 infections, while the remaining three remained asymptomatic despite lacking vaccine-induced immunity. Regarding CLL treatment, five patients required therapy due to disease progression. Three received ibrutinib as first-line therapy, achieving complete hematological response. Two patients obtained partial response, one of whom had long-standing disease and multiple relapses. Notably, one patient experienced spontaneous disease control without requiring anti-leukemic therapy following IVIg-GAM initiation. The IVIg-GAM was well-tolerated, with mild adverse events (rash and transient hypotension) observed in some patients during initial infusions. Premedication with paracetamol, dexamethasone, and diphenhydramine was administered to mitigate infusion reactions.
To our knowledge, this study is the first to evaluate infection events, antimicrobial use, and Ig levels in CLL patients receiving IVIg-GAM. Our findings show that IVIg-GAM was safe and effective in reducing infection rates and antimicrobial use in CLL patients with hypogammaglobulinemia. Larger studies are needed to confirm these findings. An updated cohort follow up will be presented at the meeting.
Keywords : infections
hypogammaglobulinemia
IVIg-repleacement-therapy
Please indicate how this research was funded. :
Please indicate the name of the funding organization.: